
AMH and its Significance?
-Dr.Shruti Mane , Fertility & IVF consultant
AMH also known as Anti-Mullerian hormone is a marker which gives us a value of ovarian reserve in females.
Ovarian reserve reflects the quantity and quality of available oocytes in the females and also has become an indispensable measure for understanding a women’s reproductive potential aka her biological clock.
AMH levels are now routinely done as any other hormonal analysis to understand the fertility potential of the women. It also helps in deciding the treatment modality needed for the couple in patients undergoing medically assisted reproductive technology ; and in the diagnosis of ovarian failure, polycystic ovarian syndrome, and granulosa cell tumour.
Anti-Mullerian hormone (AMH) is produced by the granulosa cells of primary, preantral, and small antral follicles in the ovaries. AMH can be tested on any day of menstrual cycle.
The quantitative measurement of serum AMH levels has revealed that ovarian reserve may vary in women of the same chronological age.
Moreover, we can safely say that AMH is the most reliable marker of ovarian reserve, which may be useful for a wide range of clinical applications including the optimization of fertility treatments, the diagnosis of disorders of reproductive endocrinology, and the assessment of ovarian toxicity due to medical and surgical treatments.
Salpingectomy and uterine artery embolization, which is a fertility-preserving intervention in cases of postpartum haemorrhage, may have lasting effects on blood flow to the ovaries, leading to a decline in ovarian reserve.
Serum AMH levels become undetectable within 5 years before menopause.
Serum AMH when paired with Antral follicle count of ovaries done on day 2/3 of the menstrual cycle by transvaginal ultrasound gives the most accurate estimate of a females ovarian reserve and reproductive potential.
Implications and limitations of measurements of serum anti-Mullerian hormone (AMH) levels in various clinical conditions
Clinical scenarios |
What have we learned?
|
What should we know?
|
Medically assisted reproduction
| Good correlation to oocyte yield Predictive potential for poor and hyper-response
| Predictive potential for live births. Optimization of protocols to improve treatment success
|
General population
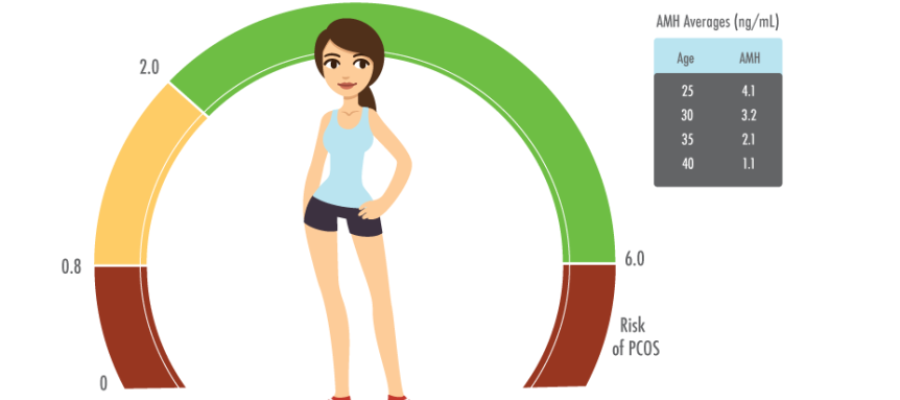
| Peaks around 25 years of age and gradually declines Very low serum AMH level does not necessarily mean sterility
| Predictive potential for future fertility
|
Menopause/POI (Premature ovarian Insufficiency)
| Undetectable serum AMH level is followed by menopause within a certain time period depending on Age
| Selection and diagnosis of subclinical POI
|
PCOS
| Elevated serum AMH level is correlated with severity
| Association with pathophysiology Optimization of treatment schedules according to serum AMH levels
|
Ovarian toxicity/surgical intervention
| Decline depending on chemotherapeutic regimens and surgical interventions, especially cystectomy for endometriomas
| Indication of fertility preservation( egg/embryo freezing) Optimal interventions according to ovarian reserve
|